US is an easily and widely used imaging modality as the first step tool in the emergency department, especi-ally in the evaluation of children and pregnant patients. But it has many limitations: sonographer dependency, obesity, abdominal gas, and ineffective ability to solve complicated disease processes
12,13. Acute abdomi-nal pain in pregnant is another challenging problem that US is generally inefficient to overcome. Lazarus et al.
14 has reported that in 30% of pregnant patients with abdominal pain in whom the US study was nega-tive, additional imaging gave important findings, with 64% of these new findings requiring surgical interven-tion. We did not use the findings of US in our study. Pregnant patients and children under 16 years old were also excluded from our study.
CT is the most commonly used modality in acute ab-dominal pain with high sensitivity and specifity over 90%. However, it is well known that, ionizing radiation and use of contrast material are the disadvantages. This results in an obstacle especially in the evaluation of pregnant patients and children15. It is also stated that ionizing radiation is causing increasing concern, both in the general population and in the medical community16. Although, abdominal CT can be performed without contrast material, it is stated that the intravenous administration of contrast material facilates the evaluation with good accuracy and a high level of di-agnostic confidence, especially in rendering diagnosis in thin patients, in whom fat interfaces may be almost absent17. In our study, we have found that CECT was more sensitive than NECT, with better accuracy rates (92.9% vs 86.3%). Our accuracy rate for all CTs in acute abdominal pain was 91.6%, compatible with the literature, whereas we had a lower sensitivity rate (53.3%) compared to a previous study in which it was reported to be generally over 90%17. This lower rate may be due to exclusion of most urinary emergencies from the study sample, exclusion of all bowel obstruc-tions, high number of complex disease processes and nonenhanced CTs. None of our patients used enteral contrast medium. It seems that lack of rectal contrast does not interfere an accurate diagnosis in acute abdo-minal pain. In a study with a series of 1021 patients, it was found that there were no inconclusive CT scans due to the lack of enteral contrast material18. Studies show that initial US followed by CT examination as a diagnostic strategy regarding acute abdominal pain, reduces unnecessary CT scans, and thus reducing ra-diation exposure19,20. All of our patients un-derwent initial US examination, followed by DW-MRI and CT scan. DW-MRI and CT was decided when US was either inefficient or a further diagnostic modality was needed on the basis of clinical and laboratory evaluation. In our study, in patients who were found to have acute appendicitis at initial US, CT was not per-formed, and these patients were excluded from the study. This was also applicable for patients who were diagnosed as acute cholecystitis at initial US. DW-MRI and CT imaging were obtained in these patients when the clinical picture and laboratory results (e.g. high liver function tests and amylase levels) pointed cholan-gitis or pancreatitis, as in 22 patients in our study. Ele-ven of them were found to be cholecystitis, 2 cholecys-titis with cholangitis, and 9 pancreatitis. Patients with hydroureteronephrosis at initial US had NECT without DW-MRI, and therefore they were excluded from the study. We had a total of 17 patients with acute pyelo-nephritis. Initial US evaluation of these patients did not show prominent degree of hydroureteronephrosis or give enough information regarding the clinical status, so DW-MRI and CT imaging were obtained.
There are also many attempts to decrease the radiation dose in CT scans and many studies have been publis-hed regarding this issue, so far17. Exposure to ioni-zing radiation is a disadvantage of CT. The dose of radiation associated with abdominal CT in acute abdo-men is approximately 10 mSv. It is estimated that, for a 25 year old patient, the risk of cancer induction for such a CT scan is about 1 in 900, the risk of fatal can-cer induction is 1 in 1800; for a 50 year old, the equivalent risks are 1 in 1500 and 1 in 2500, respectively21,22. In general, consensus exists that the information obtained with diagnostic CT outweighs the risk associ-ated with radiation and that the risk of cancer induction should be seen in the light of the lifetime cancer risk18.
There are many studies in the literature reporting the use of MRI for management of acute abdominopelvic pain. Recent advances in MRI hardware and software have allowed the development of rapid imaging tech-niques that are particularly applicable for emergency department indications23-25. Although CT scanning is the primary imaging method used in the emergency department, MRI is increasingly being used for acute abdominal pain. Being free of ionizing radiation and no need of iodinated contrast medium are the advantages of MRI. Furthermore, a majority of acute abdominopelvic diseases dont require the use of intravenous contrast medium1,17,24-26. Abdominal DW-MRI has been increasingly used with improvements in tech-nology and MRI instrumentation since 1990s. It is well known that DW-MRI relies on the principle of diffe-rent degrees of mobility of molecules, primarily water molecules, among different tissues at cellular level. Tissue cellularity, cell membrane integrity, types of macromolecules present, perfusion level, and physi-cochemical properties affect the diffusion of water molecules1,25. Diffusion is inversely related to cellularity, cell membrane integrity and lipophilicity. Restricted diffusion is observed in tissues with high cellularity (tumors, abscesses, fibrosis and cytotoxic edema)6,27-29. The images are obtained in short interval times and without the need of contrast me-dium. Quantitative analysis may be performed with the generation ADC maps from diffusion images obtained at different b values27. Although at least two b va-lues are required for DW imaging analysis, it is stated that the application of a greater number of b values will improve the accuracy of the calculated ADC30 In our study, we used 0, 500, and 1000 s/mm2 standard b values. We did not use any contrast enhanced MRI or other MRI sequenses, in order to gain time for urgent cases.
Interestingly, our study revealed a high sensitivity, specificity, and accuracy rates for DW-MRI (94.5%, 100%, 99%, respectively) which were even higher in combined methods (100%). To our knowledge, this is the first study that covers many causes of acute abdo-minal pain with a combination of DW-MRI and CT imaging. We think that this high rates is the result of combined imaging methods. And also it is a remarkab-le point that, the final diagnosis is made by the consen-sus of three radiologists who also take account of a good clinical and laboratory based evaluation.
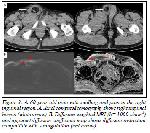
In our study, DW-MRI had also improved the diagno-sis of complex disease processes. One of them was tumoral trombus of SMV caused by hepatocellular cancer (HCC) invasion (Figure. 2).

Click Here to Zoom |
Figure 2: A. 86-year-old man with abdominal discomfort, generali-zed pain for the past few days. A Dynamic contrast-enhanced axial CT images reveal the hypervascular hepatocellular carcinoma (HCC)[long White arrow], invading portal vein and leading to tumor thrombus of superior mesenteric vein (white arrow). B,C. Diffusion-weighted MRI (b= 1000 s/mm2) and apparent diffusion coefficient maps show the tumor and tumor thrombus with restricted diffusion (red arrow). D. Diffusion-weighted MRI shows ischemic changes of small bowel (star). |
CT successfully revealed the hypervascular liver tumor invading portal vein, reaching to SMV. DW-MRI both showed the malignant nature and extent of invasion as well as ischemic changes of small bowel, thus contri-buting to the diagnosis. At CT the ischemia of small bowel was occult. DW-MRI also improved the visuali-zation of the tumoral thrombus.
Our study also showed that CT was inefficient to cha-racterize pyelonephritis, especially with NECT. Two of 17 patients with pyelonephritis could be defined by CT-only reader, while 16 were diagnosed by DW-MRI-only reader, and all were diagnosed with the combination of examinations.
We have also found that in 14 intestinal ischemia with different causes, CT-only reader could show ischemic changes in 3 of them, and DW-MRI-only reader could characterize all cases of ischemia. With combined reviews, both the cause and ischemic change of intesti-ne were clearly visualized.
Similarly, in the evaluation of stranguled inguinal her-nias, DW-MRI reader diagnosed all the strangulations accompanying the inguinal hernias (Figure 3).
Click Here to Zoom |
Figure 3: A. 60-year-old man with swelling and pain in the right inguinal region. A. Axial computed tomography shows right inguinal hernia (white arrow). B. Diffusion-weighted MRI (b= 1000 s/mm2) and apparent diffusion coefficient map shows diffusion restriction compatible with strangulation (red arrow). |
We had an interesting case with right lower quadrant pain that was found to be due to right pubic bone metastasis visualized on DW-MRI, which was nonvisible at CT (Figure. 4).

Click Here to Zoom |
Figure 4: A. 67-year-old man with right lower quadrant pain due to right pubic bone metastasis. (A,B) Diffusionweighted MRI (b=1000 s/mm2) and aparent diffusion coefficient map showed restricted diffusion of right pubic bone (white arrow) and C axial CT images of pubic bone was normal. |
Relatively small number of some sample emergencies, especially those with urinary stones that is one of the most common cause of acute abdominal pain, exclu-sion of bowel obstructions, lack of a gold standart comparison method other then the final diagnosis as we called accepted diagnosis made by decision of three radiologists, and low spatial resolution of DW-MRI were our major limitations.
In conclusion, DW-MRI is a non-invasive imaging method which has no ionizing radiation, dose not requ-ire contrast media, and can be easily performed in a short time. We suggest that DW-MRI should be added to the imaging protocol for acute abdominal pain in emergency departments, especially for pregnant woman and children. DW-MRI may aid in the detec-tion of the acute focus (inflammation or infection) with its bright signal, and thus guiding a prompt diagnosis. We propose that this is especially critical when a NECT scan is planned.
DW-MRI can also have a role in monitoring patients with acute abdominal pain, who are not operated, and need a close follow up. So it can help to prevent un-necessary CTs in follow p, and thus reducing exposure of ionizing radiation.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki decla-ration and its later amendments or comparable ethical standards.


)
)
)
)
)
)
)