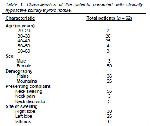
A total of 62 patients with hypoactive solitary thyroid
nodule were identified: 3 (4,8%) were male and 59
(95,2%) were females. Age of the patients ranged from
24 to 67 years with mean age of 41,4 years.
Characteristics of the patients were shown in Table
1.
Thirty six (58%) patients were from plain areas and 26 (42%) were residents of hilly areas. Commonest
presentation was neck swelling in 56 (90,3%) of the
patients. FNAC results revealed 37 (59,6%) cases as
benign lesions, 4 (6,4%) as hurthle cell tumours, 11
(17,7%) as follicular neoplasm, 2 (3,2%) as suspected
of malignancy, and 8 (12,9%) cases as papillary
carcinoma. Histopathological examination of excised
specimens showed 34 (54,8%) cases as nodular
hyperplasia, 10 (16,1%) as follicular adenoma, 2
(3,2%) as follicular carcinoma with capsular invasion,
10 (16,1%) as papillary carcinoma, 2 (3,2%) as hurthle
cell adenoma, 2 (3,2%) as hurthle cell carcinoma with
capsular invasion and, 2 (3,2%) as Hashimoto's
thyroiditis. Comparison of FNAC with
histopathological findings was performed. Thirty seven
cases were diagnosed benign lesions by FNAC. Thirty
two of these cases were nonneoplastic lesions, 2 as
follicular adenoma, 1 as follicular carcinoma and 2 as
papillary carcinoma in histopathological examination
(Table
2). Twenty five cases were diagnosed as
neoplastic lesions (hurthle cell tumours, follicular
neoplasm, suspected malignancy, and papillary
carcinoma) by FNAC. Two of these cases were
nonneoplastic lesions, 10 were benign neoplastic
lesions, 11 were carcinoma, and 2 cases of suspected
malignancy were diagnosed as Hashimoto's thyroiditis
on histopathological examination (Table
3). False
positive and false negative results were shown in Table
4. Statistical analysis of neoplastic lesions (Table
5)
showed sensitivity, specificity, accuracy, false positive
rate, false negative rate, positive predictive value, and
negative predictive value of FNAC to be 80,7%,
88,8%, 85,4%, 11,1%, 19,2%, 80,7%, and 88,8%,
respectively. Whereas statistical analysis of
carcinomatous lesions (Table
6) showed sensitivity,
specificity, accuracy, false positive rate, false negative
rate, positive predictive value, and negative predictive
value of FNAC to be 78,5%, 95,8%, 91,9%, 4,16%,
21,4%, 78,5%, and 95,8%, respectively. A total of 14
cases of solitary thyroid nodules were diagnosed as detected was papillary carcinoma, 10 out of 14
(71,4%).
Click Here to Zoom |
Table 1: Characteristics of the patients presented with clinically
hypoactive solitary thyroid nodule. |

Click Here to Zoom |
Table 2: Nonneoplastic lesions diagnosed by FNAC and their comparison with histopathological diagnosis. |

Click Here to Zoom |
Table 3: Benign or suspicious neoplastic lesions diagnosed by FNAC and their comparison with histopathological diagnosis. |


)
)
)
)
)
)
)