Socio-Demographic Background of the Teenagers
and Their Caretakers
About half of the pregnant teenagers were in the third
trimester of their pregnancy which could result from
the fact that the study was carried out at ANC outlets
where pregnant women in developing countries are
known to normally book late
11. The high proportion
of those without education could be due to the fact that most of the respondents were coming from the surrounding
rural communities in the metropolis where
formal education is usually a challenge. This result is
consistent with other studies that have reported the
level of education to be negatively associated to the
prevalence of teenage pregnancy
11,15. About twothirds
of respondents (64.2%) were married, which is
also consistent with several research findings including
the UNICEF-sponsored International Planned Parenthood
Federation (IPPF) report on child marriage
21.
As shown in Table 1, many of the caretakers were
between their late 20s to early 30s and were mostly
males (83.7%) because most of the teenagers were
married and were living with their husbands. Again,
many of the caretakers (70.3%) had no education
which further confirms the findings that education of
the spouses and not only that of the teenager could
have a negative effect on the occurrence of teenage
pregnancies since those who are not in school tend to
marry earlier than their literate counterparts22. Almost
all the caretakers (87.0%) were in informal employment
(Table 3).
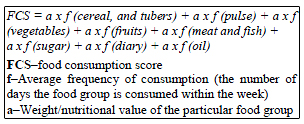
Dietary Intake of the Pregnant Teenagers
Among all the eight food groups, which were used to
estimate the levels of food intake with the Food Consumption
Scores (FCS), staples (cereal grains, roots
and tubers) were the highly consumed food group with
a mean weekly frequency of 6 days. This was followed
by Fats and sugars, with 5 and 4 days per week respectively
as their mean weekly frequencies of intake, were
the next mostly consumed food groups. The least consumed
food groups were vegetables and fruits (Table
5). This pattern is consistent with dietary patterns of
populations in developing countries which are mainly
composed of staples and energy dense food groups
(fats and oil) and a limited quantity of animal products
and fresh fruits and vegetables23,24. This presents
a risk of deficiencies or excesses of several micro or
macronutrients25. The low consumption of fruits and
vegetables as well as meat and fish presents a nutritional
concern especially with respect to micronutrient
adequacy of their diet, as these nutrients are essential
during pregnancy especially among teenagers.
The mean Composite Food Consumption Score
(CFCS) was 42.9, which is at the extreme lower end
for the acceptable level of intake. Despite this lower
mean CFCS, about half of the teenagers (51.7%) had
an acceptable level of food intake based on the
FAO/WFP CFCS thresholds. Not much difference was
observed in the proportions at borderline (27.2%) and
unacceptable (21.1%) levels of food intake (Figure 1).
Dietary Quality of the Pregnant Teenagers
With regard to the quality of diet which was measured
with the IDDS, it was observed that out of a total of 12
food groups, the respondents consumed averagely from
10 different food groups (Table 6). This means that
generally the respondents had good quality diet because
previous studies have reported dietary diversity
as an important element of a high quality diet26,27. They therefore have a greater probability of meeting
their energy and micronutrient requirements as Dietary
Diversity Score have been reported by many studies to
be correlated positively with energy and micronutrient
intake28-32.
The Effects of the Socio-Demographic and Economic
Factors on the Dietary Intake
Among all the socio-demographic variables of the
teenagers, none except the term of their pregnancies,
had significant associations with their level of food
intake (Figure 2 and Table 7). This association could
be explained by the fact that these teenagers are mainly
dependent on their caretakers and as such obtained
their food from them. Those in their second trimester
had highest proportion of those with acceptable intake.
This could be due to the aversions and other non-diet
friendly symptoms of early pregnancy such as nausea
and appetite loss that often affect food intake during
the first trimester33. Also, within this period, the
teenager is still in a transition from her normal life to
life during pregnancy and as such the nutritional support
offered to her due to the pregnancy is yet to start11,34,35.

Click Here to Zoom |
Table 7: Significant associations of some socio-demographic variables with level of food intake |
The significant associations observed between
gender of the caretakers and their relationship with the
respondents (Table 7) could be due to the fact most of
them were married and thus were staying with their
husbands. Occupational status that was used as a measure
of economic status of the caretakers was also significantly
associated with levels of food intake. This is
consistent with the age-old literature that occupation is
associated positively with economic food acquisition or
accessibility of households or individuals36,37.
Even though the overall food consumption and dietary
diversity or quality of the pregnant teenagers was acceptably
high, a considerable proportion still fell within
both the poor and borderline food consumption categories
intake. The food consumption was observed to be
significantly associated with the caretakers sociodemographic
factors such as gender, relationship with
the teenager and occupation.
These findings highlight the need consider the
caretakers or spouses of pregnant teenagers in designing
intervention programs and policies to improve the
dietary intake of pregnant teenagers for the improvement
and maintenance of their nutritional status during
and after pregnancy. These programs and policies will
go a long way to reduce the contribution of teenage
pregnancy on maternal and infant mortalities and morbidities
in the metropolis and the country and beyond.


)
)
)
)
)
)
)
)
)